Our two lungs provide a large surface area for the exchange of gas with the air around us. The alveoli of the lung provide this exchange surface, where the air can come into close association with the circulation. The alveoli are joined by a series of bronchioles and bronchi to the trachea that communicates with the environment via the oral and nasal cavities. The gases exchanged; Oxygen and Carbon Dioxide are carried in the blood by various means around the body to or form the lungs.
 The bronchioles are less than one millimetre
in diameter, unlike the rigid bronchi, they have no cartilage support. The epithelium is of a simple columnar ciliated
type with only a few goblet (mucus secreting) cells. Surrounding this is a smooth muscle layer that spirals around the
bronchioles. The bronchioles split up into terminal bronchioles and then respiratory bronchioles that are connected to
the alveolar sacs by alveolar ducts. Alveolar sacs each give rise to individual alveoli, this is where most gaseous
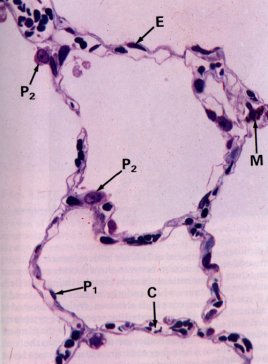
exchange takes place. Alveoli consist of surface epithelium, supporting tissue and blood vessels (mainly capillaries
[C]). The surface epithelium is made up of Type I pneumocytes [P1] (lining cells) and Type II pneumocytes
[P2] which secrete surfactant. Surfactant reduces surface tension within the alveoli preventing alveolar
collapse during expiration.
The bronchioles are less than one millimetre
in diameter, unlike the rigid bronchi, they have no cartilage support. The epithelium is of a simple columnar ciliated
type with only a few goblet (mucus secreting) cells. Surrounding this is a smooth muscle layer that spirals around the
bronchioles. The bronchioles split up into terminal bronchioles and then respiratory bronchioles that are connected to
the alveolar sacs by alveolar ducts. Alveolar sacs each give rise to individual alveoli, this is where most gaseous
exchange takes place. Alveoli consist of surface epithelium, supporting tissue and blood vessels (mainly capillaries
[C]). The surface epithelium is made up of Type I pneumocytes [P1] (lining cells) and Type II pneumocytes
[P2] which secrete surfactant. Surfactant reduces surface tension within the alveoli preventing alveolar
collapse during expiration.
Each Lung has a blunt apex, which projects up into the neck for about 2.5cm above the clavicle; a concave base that sits on the diaphragm; a costal surface corresponding to the chest wall; and a concave mediastinal surface, which is moulded to the pericardium and other mediastinal structures. The hilum is where various structures (bronchi, vessels and nerves) forming the root of the lung, communicate with the lung. It is found at the middle of the mediastinal surface.
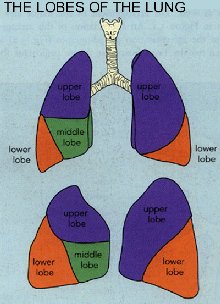 The lungs are separated into lobes by fissures,
the left lung is separated by the oblique fissure, running from the base upward and backward across the medial and
costal surfaces until it cuts the posterior border approximately 6cm below the apex. This gives the left lung two
lobes (upper and lower). The right lung is separated by an additional horizontal fissure, giving it three lobes,
the additional lobe is called the middle lobe.
The lungs are separated into lobes by fissures,
the left lung is separated by the oblique fissure, running from the base upward and backward across the medial and
costal surfaces until it cuts the posterior border approximately 6cm below the apex. This gives the left lung two
lobes (upper and lower). The right lung is separated by an additional horizontal fissure, giving it three lobes,
the additional lobe is called the middle lobe.
The lungs are each divided into ten anatomical, functional and surgical bronchopulmonary segments. Each segment is the subdivision of lung that is supplied by a segmental bronchus, segmental artery, autonomic nerves and lymph vessels. Venous drainage to each segment is via the segmental vein, which runs in the connective tissue between adjacent segments. Individual segments can be removed surgically if diseased.
The lung connective tissue, bronchi and pleura receive their blood supply from the bronchial arteries which branch from the aorta, blood drains into the azygos and hemiazygos vein via the bronchial veins.
The lymph structure of the lungs is important, as it is a significant route of metastatic spread.
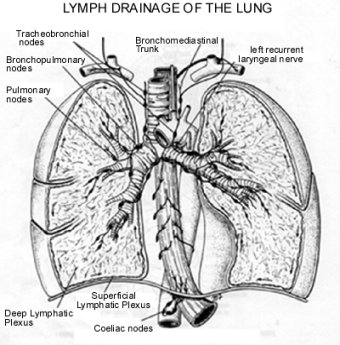 The lymph vessels originate in
superficial and deep plexuses. The deep plexus drains the deeper lung structures, travelling along the bronchi
and pulmonary vessels, it communicates with pulmonary nodes in the lung which in turn drain into the bronchopulmonary
nodes in the hilum. The superficial plexus lies beneath the visceral pleura and drains the surface of the lung and
then drains into the bronchopulmonary nodes. The bronchopulmonary nodes drain out of the hilum into the tracheobronchial
nodes and then into the bronchomediastinal lymph trunks.
The lymph vessels originate in
superficial and deep plexuses. The deep plexus drains the deeper lung structures, travelling along the bronchi
and pulmonary vessels, it communicates with pulmonary nodes in the lung which in turn drain into the bronchopulmonary
nodes in the hilum. The superficial plexus lies beneath the visceral pleura and drains the surface of the lung and
then drains into the bronchopulmonary nodes. The bronchopulmonary nodes drain out of the hilum into the tracheobronchial
nodes and then into the bronchomediastinal lymph trunks.
The lungs are surrounded by the ribcage. The ribcage and associated muscles facilitate expansion of the lungs for inspiration and the relaxation required for expiration. These two repeated actions serve to refresh the air in the lungs to permit efficient gaseous exchange. Inspiration is achieved by expansion of the ribcage and lowering of the diaphragm. Ribcage expansion is usually achieved by the action of the scaleni muscles of the neck and the intercostal muscles. Under heavier breathing and particularly when in respiratory distress, these muscles are assisted by other accessory muscles; sternocleidomastoid, trapezius, levator scapulae, rhomboid muscles, serratus anterior and pectoralis minor. Expiration is usually facilitated by elastic recoil, but under stressful situations forced expiration, involving the quadratus lumborum, serratus posterior and latissimus dorsi takes place.
RETURN TO CONTENTS PAGE
Next section: Pathology: Process and Classification